The mandible, being one of the most prominent and mobile bones of the facial skeleton, is highly susceptible to traumatic injuries. Mandibular fractures represent a significant proportion of maxillofacial trauma cases, often resulting from road traffic accidents, assaults, falls, or occupational injuries. The present study, titled “Clinicoradiological Study of Mandibular Fractures in Tertiary Care Centre”, aims to analyze in detail the etiology, clinical presentation, radiological patterns, and types of mandibular fractures encountered in a tertiary care setting in the span of two years (October 2023 - October 2025). Special emphasis is placed on the diagnostic role of clinicoradiological correlation in accurate localization and classification of fractures. Furthermore, the study evaluates different management modalities, ranging from conservative approaches such as closed reduction and maxillomandibular fixation to surgical interventions like open reduction and internal fixation. By comparing outcomes of these treatment strategies, the study seeks to highlight the practical considerations, challenges, and effectiveness of both conservative and surgical methods in routine clinical practice.
| Published in | International Journal of Clinical Oral and Maxillofacial Surgery (Volume 12, Issue 1) |
| DOI | 10.11648/j.ijcoms.20261201.11 |
| Page(s) | 1-6 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2026. Published by Science Publishing Group |
Mandibular Fractures, Maxillofacial Trauma, Clinicoradiological Evaluation, Conservative Management, Surgical Treatment
Category | Subcategory | Percentage (%) |
|---|---|---|
Age Group (years) | 20–40 | 62% |
0–19 | 18% | |
41 & above | 20% | |
Etiology | Road Traffic Accidents | 58% |
Accidental Falls | 25% | |
Interpersonal Assaults | 17% | |
Fracture Site | Condylar Region | 34% |
Parasymphysis | 28% | |
Symphysis | 22% | |
Ramus | 16% | |
Treatment Modality | ORIF (Miniplates) | 61% |
Conservative (IMF/Dietary) | 39% |
RTA | Road Traffic Accident |
OPG | Orthopantomogram |
CT | Computed Tomography |
ORIF | Open Reduction and Internal Fixation |
MMF | Maxillomandibular Fixation |
IMF | Intermaxillary Fixation |
ENT | Ear, Nose and Throat |
TMJ | Temporomandibular Joint |
| [1] | Rai A, Karwal V, Nigam S, Saxena A, Sharma M. Outcome study of mandibular fractures treated by surgical stabilization with plates and screws. Cureus. 2024; 16(4): e58561. |
| [2] | Oxford M, Tucker J, Goldenberg D, King TS, Ziai K, Henry C, Lighthall JG. Comparison of pediatric and adult mandibular fractures: identifying differences in presentation and management using a national trauma database. J Craniofac Surg. 2025; 36(2): 461–464. |
| [3] | Roccia F, Cena P, Cremona G, Garzino Demo P, Sobrero F. Characteristics and surgical management of bilateral body mandibular fractures: a 23-year experience. J Clin Med. 2025; 14(1): 160. |
| [4] | Mudawi AIAA. Mandibular fractures: a five-year retrospective review. Egypt J Health Care. 2025; 16(3): 845–852. |
| [5] | Kawilarang B, Sanjaya IGPH, Hariantana AR. A five-year epidemiological analysis of mandible fractures in Bali. Jurnal Plastik Rekonstruksi. 2025; 12(1): 7–13. |
| [6] | Khan W, Syed K, Khan S, Safwan AA, Saboor A, Khan A, Rahim M. Outcome of open reduction and internal fixation using one titanium plate and arch bar for mandibular fractures in symphyseal and parasymphyseal region. J Gandhara Med Dent Sci. 2025; 12(4): 53–57. |
| [7] | Vetter JD, Topazian RG, Goldberg MH, Smith DG. Facial fractures occurring in a medium-sized metropolitan area: recent trends. Int J Oral Maxillofac Surg. 2019; 48(11): 1411–1418, |
| [8] | Boffano P, Kommers SC, Roccia F, Forouzanfar T. Mandibular trauma: a two-century review. Int J Oral Maxillofac Surg. 2015; 44(12): 1389–1399. |
| [9] | Kumar N, Yadav SK, Tandon R, Chandra A. Management of pediatric mandibular fractures: a review. Natl J Maxillofac Surg. 2020; 11(1): 3–9. |
| [10] | Champy M, Loddé JP, Schmitt R, Jaeger JH, Muster D. Mandibular osteosynthesis by miniature screwed plates via a buccal approach. J Maxillofac Surg. 1976; 4(1): 14–21. |
| [11] | Al-Ahmed HE, Jaber MA, Fanas SH, Karas M. The pattern of maxillofacial fractures in Sharjah, United Arab Emirates: a review of 230 cases. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2004; 98(2): 166-170. |
| [12] | Lee KH. Global trends in maxillofacial fractures. Craniomaxillofac Trauma Reconstr. 2008; 1(1): 31-36. |
| [13] | Rowe NL, Killey HC. Fractures of the Facial Skeleton. Edinburgh: Churchill Livingstone; 1968. |
| [14] | Ellis E, Moos KF, el-Attar A. Ten years of mandibular fractures: an analysis of 2,137 cases. Oral Surg Oral Med Oral Pathol. 1985; 59(2): 120-129. |
| [15] | F. Roccia, P. Cena, G. Cremona, P. Garzino Demo, and F. Sobrero, “Characteristics and Surgical Management of Bilateral Body Mandibular Fractures: A 23?Year Experience,” J. Clin. Med., vol. 14, no. 1, article 160 (pp. 1–15), 2025. |
| [16] | Chrcanovic BR. Factors influencing the incidence of maxillofacial fractures, Oral Maxillofac Surg. 2012; 16(1): 3–17. |
| [17] | Haug RH, Prather J, Indresano AT. An epidemiologic survey of facial fractures, J Oral Maxillofac Surg. 1990; 48(9): 926–932. |
| [18] | Madison Oxford, Jacqueline Tucker, Dana Goldenberg, Tonya S. King, Kasra Ziai, Cathy Henry, and Jessyka G. Lighthall, “Comparison of Pediatric and Adult Mandibular Fractures: Identifying Differences in Presentation and Management Using a National Trauma Database,” J. Craniofac. Surg., vol. 36, no. 2, pp. 461–464, 2025. |
| [19] | Brasileiro BF, Passeri LA. Epidemiological analysis of maxillofacial fractures in Brazil, J Oral Maxillofac Surg. 2006; 64(7): 1019–1024. |
| [20] | Dongas P, Hall GM. Mandibular fracture patterns in Tasmania, Australia, Aust Dent J. 2002; 47(2): 131–137. |
| [21] | Kroon FH, Mathisson M, Cordey JR, Rahn BA. The use of miniplates in mandibular fractures, J Craniomaxillofac Surg. 1991; 19(5): 199–204. |
| [22] | Adeyemo WL, Ladeinde AL, Ogunlewe MO, James O. Trends and characteristics of oral and maxillofacial injuries in Nigeria: a review of the literature. Head Face Med. 2011; 7: 6. |
| [23] | Posnick J. C. Pediatric facial fractures: evolving patterns of treatment, J Oral Maxillofac Surg. 2000; 58(2): 136–147. |
| [24] | Ellis E, Walker L. Treatment of mandibular angle fractures using one noncompression miniplate, J Oral Maxillofac Surg. 1996; 54(7): 864–871. |
| [25] |
Ellis E. Treatment methods for fractures of the mandibular angle, Int J Oral Maxillofac Surg. 1999; 28(4): 243–252.
HYPERLINK "
https://doi.org/10.1016/S0901-5027(98)01520-9" https://doi.org/10.1016/S0901-5027(98)01520-9 |
APA Style
Gujrathi, A. B., Paikrao, Y. M., Rewatkar, A. K. (2026). Clinicoradiological Study of Mandibular Fractures in Tertiary Care Centre. International Journal of Clinical Oral and Maxillofacial Surgery, 12(1), 1-6. https://doi.org/10.11648/j.ijcoms.20261201.11
ACS Style
Gujrathi, A. B.; Paikrao, Y. M.; Rewatkar, A. K. Clinicoradiological Study of Mandibular Fractures in Tertiary Care Centre. Int. J. Clin. Oral Maxillofac. Surg. 2026, 12(1), 1-6. doi: 10.11648/j.ijcoms.20261201.11
@article{10.11648/j.ijcoms.20261201.11,
author = {Atishkumar Balajirao Gujrathi and Yogesh Madhaorao Paikrao and Awantika Kishor Rewatkar},
title = {Clinicoradiological Study of Mandibular Fractures in Tertiary Care Centre},
journal = {International Journal of Clinical Oral and Maxillofacial Surgery},
volume = {12},
number = {1},
pages = {1-6},
doi = {10.11648/j.ijcoms.20261201.11},
url = {https://doi.org/10.11648/j.ijcoms.20261201.11},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijcoms.20261201.11},
abstract = {The mandible, being one of the most prominent and mobile bones of the facial skeleton, is highly susceptible to traumatic injuries. Mandibular fractures represent a significant proportion of maxillofacial trauma cases, often resulting from road traffic accidents, assaults, falls, or occupational injuries. The present study, titled “Clinicoradiological Study of Mandibular Fractures in Tertiary Care Centre”, aims to analyze in detail the etiology, clinical presentation, radiological patterns, and types of mandibular fractures encountered in a tertiary care setting in the span of two years (October 2023 - October 2025). Special emphasis is placed on the diagnostic role of clinicoradiological correlation in accurate localization and classification of fractures. Furthermore, the study evaluates different management modalities, ranging from conservative approaches such as closed reduction and maxillomandibular fixation to surgical interventions like open reduction and internal fixation. By comparing outcomes of these treatment strategies, the study seeks to highlight the practical considerations, challenges, and effectiveness of both conservative and surgical methods in routine clinical practice.},
year = {2026}
}
TY - JOUR T1 - Clinicoradiological Study of Mandibular Fractures in Tertiary Care Centre AU - Atishkumar Balajirao Gujrathi AU - Yogesh Madhaorao Paikrao AU - Awantika Kishor Rewatkar Y1 - 2026/01/29 PY - 2026 N1 - https://doi.org/10.11648/j.ijcoms.20261201.11 DO - 10.11648/j.ijcoms.20261201.11 T2 - International Journal of Clinical Oral and Maxillofacial Surgery JF - International Journal of Clinical Oral and Maxillofacial Surgery JO - International Journal of Clinical Oral and Maxillofacial Surgery SP - 1 EP - 6 PB - Science Publishing Group SN - 2472-1344 UR - https://doi.org/10.11648/j.ijcoms.20261201.11 AB - The mandible, being one of the most prominent and mobile bones of the facial skeleton, is highly susceptible to traumatic injuries. Mandibular fractures represent a significant proportion of maxillofacial trauma cases, often resulting from road traffic accidents, assaults, falls, or occupational injuries. The present study, titled “Clinicoradiological Study of Mandibular Fractures in Tertiary Care Centre”, aims to analyze in detail the etiology, clinical presentation, radiological patterns, and types of mandibular fractures encountered in a tertiary care setting in the span of two years (October 2023 - October 2025). Special emphasis is placed on the diagnostic role of clinicoradiological correlation in accurate localization and classification of fractures. Furthermore, the study evaluates different management modalities, ranging from conservative approaches such as closed reduction and maxillomandibular fixation to surgical interventions like open reduction and internal fixation. By comparing outcomes of these treatment strategies, the study seeks to highlight the practical considerations, challenges, and effectiveness of both conservative and surgical methods in routine clinical practice. VL - 12 IS - 1 ER -
Department of Ear, Nose and Throat, Dr Shankarrao Chavan Government Medical College, Nanded, India
Department of Ear, Nose and Throat, Dr Shankarrao Chavan Government Medical College, Nanded, India
Department of Ear, Nose and Throat, Dr Shankarrao Chavan Government Medical College, Nanded, India
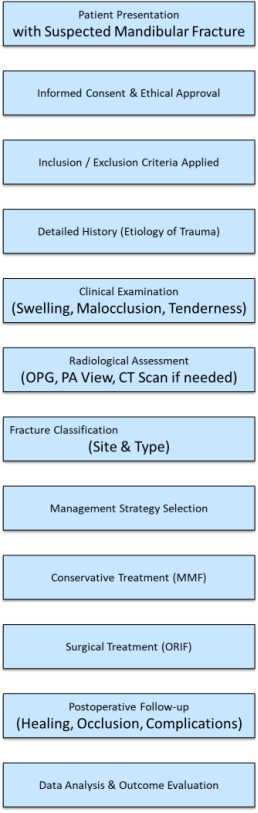
Figure 1. Flow chart of methodology.
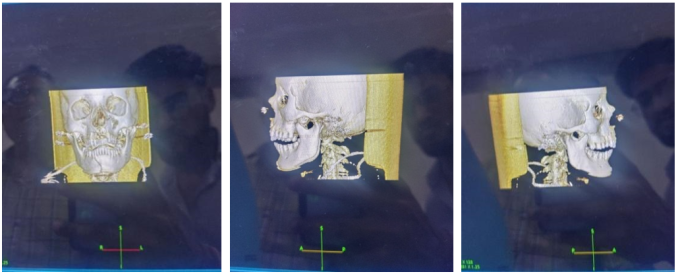
Figure 2.
Demographic pattern seen in the patient.
